
Buluba Hospital, Uganda.
December 2017.
By Renate Hoare.
Why choose Uganda? As a child who grew up in Africa, there has always been a hankering to return and give something back.
Armed with knowledge from previous work in the humanitarian field, I knew of many internet forums and Aid Organisations who were looking for radiographers. I have volunteered with Rotary Doctors in the past and so I reached out to them for guidance. My only request was to go somewhere dry. A few places were offered and I based my decision on a simple choice of where could I make a small impact with my skills in a short time frame and so with the support of the Rotary Doctor Bank of GB and Ireland, I visited Buluba.
Buluba Hospital Facts.
Buluba is located in the Mayuge District of Eastern Uganda, with the nearest town, Iganga, 22 km away and the airport a bumpy 5 hour car journey by road.
Buluba Hospital, previously known as St Francis Hospital, was founded by Catholic Missionaries in 1934, to serve as a leprosarium. The hospital and grounds cover a large land area and serve an ever increasing population of 1.94 million. The official language is Lusoga, however, the staff and most visitors speak a wonderful combination of English, Kiswahili and German.
After a 16 hour flight, a 2 hour Ugandan immigration process and 5 hour car ride, I was happy that I and my 78 kg of donated X-ray equipment had made it. This was to be my home and work for the next fortnight.


A normal day at work.
I quickly learned that there is no normal day. A siren marks the start of each working week and is the signal for both the beginning of the lunch period and end of the day. Upon hearing it for the first time, I instinctively ducked, thinking it was an earthquake siren. Formal introductions were made 5 minutes before the Monday morning clinical team gathering, where I was quickly updated on patient admissions from the weekend and activities for the upcoming week. The words that came to my mind were “there’s nothing like jumping in at the deep end”.
Visiting the various departments, I noticed how quiet and calm everything appeared. Wards and departments are spread out, with patients and staff seemingly oblivious to the distances. The lack of basic resources and adequate funding to improve many of the wards and equipment was clearly obvious and whereas I could look at it as tragic, it was actually more empowering to see how little you need to do great work. Most of the staff multitask and regardless of the struggles or lack of resources, keep a smile on their faces. There is a great sense of compassion for the patients and there are activities from cooking to washing and the constant use of cell phones taking place under every tree or in every corner with shade.
Donated equipment.

Not knowing what to expect before my visit, I reached out to radiographers who had previously volunteered overseas and was amazed at the plethora of useful tips and information available for effective donations. Donations were generously given by past Doctor Bank volunteers with experience in the field, World Radiography Trust Foundation and colleagues at work. This all amounted to 78 kilos of luggage!
Donations.
A full-length lead coat, lead gonad shields, thyroid shields, X-ray markers, marker pens, ultrasound books, diagnostic imaging texts, imaging guides, a lightbox viewing station, a pelvimetric scale and instructions, boxes of gloves, first aid kits, goggles tools and 20 Agfa Fast Cassettes of various sizes.
Powerpoint presentations given:
OPD Doctors
In preparing for my visit, I spent several days with 2 reporting radiographers, who kindly prepared me to give simple presentations on the following topics:
- Abdominal radiography interpretation
- Introduction to chest imaging
- Radiation protection
The dedicated team of clinical officers, doctors and nurses were keen to have some basic chest imaging and radiation protection training in their lunch times. During the day, I spent time with the clinical team in outpatients, amongst the noise and general patient admissions, to watch slide shows, discuss technique and talk about the hopes and dreams for Buluba. Radiation protection was by far the most popular talk. There was a fear of radiation and thus x-rays in general. It took a lot of convincing and help from Google to show that x-rays only go in the direction of the tube, they do not linger in a room and that lead coats prevent x-ray penetration.
Radiographer Training:
There is only 1 radiographer in Buluba and other than training for 5 months, over 15 years ago, he has become a self-taught enthusiastic radiographer. On the multiple occasions when the mains power was down, Moses and I had no way to x-ray patients, so we worked together, using our combined work and life experiences to extend our continuous professional development in the following areas
- Abdominal radiography interpretation
- Introduction to chest imaging
- Radiation protection
- Imaging of the appendicular skeleton
- Imaging the shoulder and the importance of the second view
- Common fractures and basic diagnosis using the red dot system
- Infection control
- Paediatric chest imaging, Erect rather than Supine
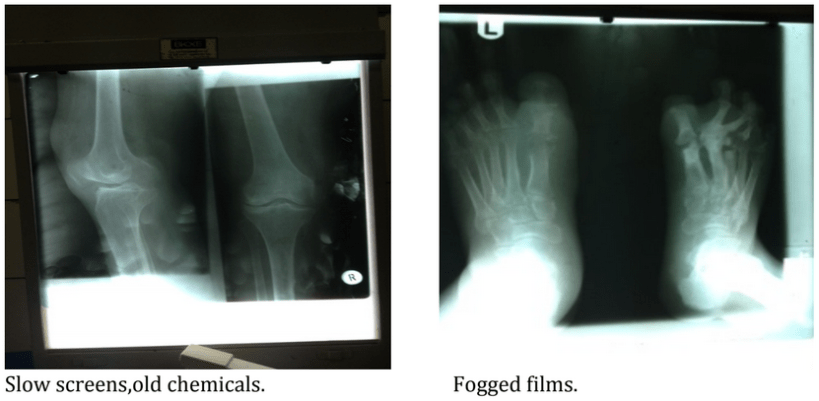
All diagnostic images now have a radiopaque marker and all extremities are imaged with both an AP and Lateral view. Using past images and those taken during my first week, we were able to create updated exposure charts for both adults and children. These are now not only stored in Moses’ head but in his office for future radiographers. Some of our early films were diagnostically poor quality due to the processing chemicals natural oxidation and age. The greater the agitation in the water tank, the dirtier the films were getting so our solution was to wash the excess fixer off films under the one running water tap. The darkroom is based adjacent to the x-ray room and with no ventilation it doesn’t take long for the fumes to accumulate and leaving your taste buds struggling to comprehend.

Challenges:
Being the only radiographer, Moses single-handedly runs the service 360 days a year. Even he can’t remember the last time he took leave. There is no radiologist for image reporting and clinical decisions are reliant on the hardworking clinical team of doctors diagnosing the x-ray images.
Although the hospital has a generator it is not capable of maintaining the x-ray service and patients either wait all day in hope of the mains power returning or come back on a later date. There are those who simply have too far to travel and opt to go without this basic diagnostic tool. Limited supplies of chemicals and film, based on funding and country imports, provide a further challenge in both providing the service and choice of treatment pathways. Each patient pays 1500 shillings (about 30p) per film which itself is a struggle to find as most are subsistence farmers. This means that nearly all patients only have 1 view on the 1 film.
Together, Moses and I created a method whereby all extremities can be imaged on a single film, regardless of the film size available, with both an AP and lateral view.
The darkroom consists of a single wet tank with developer and fixer and 1 water outlet. The 1 darkroom light was small but worth its weight in gold. Replacement bulbs are difficult to source and in the past Moses has developed films without light for 5 months. A major issue for health and safety of the radiographer was the complete lack of any darkroom ventilation. The hand processed films are mounted on drying racks which are then hung in the film drying cabinet, reliant upon mains power which is limited at best. 20 minutes after arriving in the x-ray room, patients depart carrying their film in a handmade newspaper envelope.
Urgent trauma cases requiring x-rays in times of power outages, are referred to other hospitals in the district, that are at least 2 hours away by car. This is an additional cost that most patients struggle to afford, if at all. The hospital team is extremely generous and during my time on site, I saw several cases where the community of staff pitched in or found a solution for urgent referral costs. Without this support, patients would simply not survive. Engineering maintenance and equipment quality control are reliant on the local hospital engineer, whose tasks also include managing the 1 onsite generator and the entire electrical system including most of the hospital equipment.
X-ray equipment
Current equipment consists of a Siemens Multix Ease fixed over couch x-ray tube, 1 floating top table with under table bucky and 1 erect standalone bucky.
There is no up and down movement of the table, with patients having to climb on to the table. There is no radiopaque mattress, sand bags or foam positioning aids. Whilst we take for granted the technology of the modern NHS, it was the simple things, such as a step, which patients were grateful for in Buluba. From patients with broken bones and leprosy, there was never a complaint, just a smile.
The tube has lateral movement and can be rotated 45 degrees to use with the erect chest stand. There is, however, no horizontal tube movement which results in all patients being pushed or pulled into position on the table. The erect bucky is functional, even though the brake and lock are both broken and as yet there is no spare part available.
Financial constraints in the past year have meant that there was no light beam diaphragm, once the bulb blew, until a replacement was found. This did not interrupt the service provided, as Moses guestimated the light beam diaphragm coverage.
I experienced so many scenarios that radiographers no longer face in the modern CR/DR department and enjoyed every minute of them.




Ultrasound
This service is limited to basic abdominal sonographer and obstetrics, using a Sonoscope Model A6 with variable curvilinear probe 2-7.5 MegaHZ. Currently there is 1 sonographer who visits twice a week. He scans and prepares reports for all patients and works with no breaks. Working with him for 8 hours, I realised he hadn’t even stopped for a drink.
Patients are often alone in the room with the male sonographer and it is not uncommon for them to be naked from the waist up. Men and women alike have no concerns in terms of preserving their dignity or embarrassment at the lack of gowns.
The sonographer was delighted to hear that I was a radiographer, yet dismayed that I was unable to perform ultrasonography, so he set me a challenge to get the new Siemens Sonoline Adara machine operational. This seemed a fair request and the least I could do until I got the power and input sorted and realised that everything was in German. A few tantrums and hours later, we were both pleased to announce that the operational language was now English and the scanner is fully operational. All that is needed now is another full-time sonographer.



I would like to thank the Rotary Doctor Bank, Kerry Bingham, Andy Creeden, Teresa Dawkes, Lucy Foster, Sue Marchant, Angela Ramsay, Christopher Steele, Mansel Thomas, Dr Tim Spare and the tireless devotion of all the staff, visitors and friends in Buluba.
Buluba Hospital, Uganda.
December 2017.
By Renate Hoare.
Why choose Uganda? As a child who grew up in Africa, there has always been a hankering to return and give something back.
Armed with knowledge from previous work in the humanitarian field, I knew of many internet forums and Aid Organisations who were looking for radiographers. I have volunteered with Rotary Doctors in the past and so I reached out to them for guidance. My only request was to go somewhere dry. A few places were offered and I based my decision on a simple choice of where could I make a small impact with my skills in a short time frame and so with the support of the Rotary Doctor Bank of GB and Ireland, I visited Buluba.
Buluba Hospital Facts.
Buluba is located in the Mayuge District of Eastern Uganda, with the nearest town, Iganga, 22 km away and the airport a bumpy 5 hour car journey by road.
Buluba Hospital, previously known as St Francis Hospital, was founded by Catholic Missionaries in 1934, to serve as a leprosarium. The hospital and grounds cover a large land area and serve an ever increasing population of 1.94 million. The official language is Lusoga, however, the staff and most visitors speak a wonderful combination of English, Kiswahili and German.
After a 16 hour flight, a 2 hour Ugandan immigration process and 5 hour car ride, I was happy that I and my 78 kg of donated X-ray equipment had made it. This was to be my home and work for the next fortnight.
A normal day at work.
I quickly learned that there is no normal day. A siren marks the start of each working week and is the signal for both the beginning of the lunch period and end of the day. Upon hearing it for the first time, I instinctively ducked, thinking it was an earthquake siren. Formal introductions were made 5 minutes before the Monday morning clinical team gathering, where I was quickly updated on patient admissions from the weekend and activities for the upcoming week. The words that came to my mind were “there’s nothing like jumping in at the deep end”.
Visiting the various departments, I noticed how quiet and calm everything appeared. Wards and departments are spread out, with patients and staff seemingly oblivious to the distances. The lack of basic resources and adequate funding to improve many of the wards and equipment was clearly obvious and whereas I could look at it as tragic, it was actually more empowering to see how little you need to do great work. Most of the staff multitask and regardless of the struggles or lack of resources, keep a smile on their faces. There is a great sense of compassion for the patients and there are activities from cooking to washing and the constant use of cell phones taking place under every tree or in every corner with shade.
Donated equipment.
Not knowing what to expect before my visit, I reached out to radiographers who had previously volunteered overseas and was amazed at the plethora of useful tips and information available for effective donations. Donations were generously given by past Doctor Bank volunteers with experience in the field, World Radiography Trust Foundation and colleagues at work. This all amounted to 78 kilos of luggage!
Donations.
A full-length lead coat, lead gonad shields, thyroid shields, X-ray markers, marker pens, ultrasound books, diagnostic imaging texts, imaging guides, a lightbox viewing station, a pelvimetric scale and instructions, boxes of gloves, first aid kits, goggles tools and 20 Agfa Fast Cassettes of various sizes.
Powerpoint presentations given:
OPD Doctors
In preparing for my visit, I spent several days with 2 reporting radiographers, who kindly prepared me to give simple presentations on the following topics:
- Abdominal radiography interpretation
- Introduction to chest imaging
- Radiation protection
The dedicated team of clinical officers, doctors and nurses were keen to have some basic chest imaging and radiation protection training in their lunch times. During the day, I spent time with the clinical team in outpatients, amongst the noise and general patient admissions, to watch slide shows, discuss technique and talk about the hopes and dreams for Buluba. Radiation protection was by far the most popular talk. There was a fear of radiation and thus x-rays in general. It took a lot of convincing and help from Google to show that x-rays only go in the direction of the tube, they do not linger in a room and that lead coats prevent x-ray penetration.
Radiographer Training:
There is only 1 radiographer in Buluba and other than training for 5 months, over 15 years ago, he has become a self-taught enthusiastic radiographer. On the multiple occasions when the mains power was down, Moses and I had no way to x-ray patients, so we worked together, using our combined work and life experiences to extend our continuous professional development in the following areas
- Abdominal radiography interpretation
- Introduction to chest imaging
- Radiation protection
- Imaging of the appendicular skeleton
- Imaging the shoulder and the importance of the second view
- Common fractures and basic diagnosis using the red dot system
- Infection control
- Paediatric chest imaging, Erect rather than Supine
All diagnostic images now have a radiopaque marker and all extremities are imaged with both an AP and Lateral view. Using past images and those taken during my first week, we were able to create updated exposure charts for both adults and children. These are now not only stored in Moses’ head but in his office for future radiographers. Some of our early films were diagnostically poor quality due to the processing chemicals natural oxidation and age. The greater the agitation in the water tank, the dirtier the films were getting so our solution was to wash the excess fixer off films under the one running water tap. The darkroom is based adjacent to the x-ray room and with no ventilation it doesn’t take long for the fumes to accumulate and leaving your taste buds struggling to comprehend.
Challenges:
Being the only radiographer, Moses single-handedly runs the service 360 days a year. Even he can’t remember the last time he took leave. There is no radiologist for image reporting and clinical decisions are reliant on the hardworking clinical team of doctors diagnosing the x-ray images.
Although the hospital has a generator it is not capable of maintaining the x-ray service and patients either wait all day in hope of the mains power returning or come back on a later date. There are those who simply have too far to travel and opt to go without this basic diagnostic tool. Limited supplies of chemicals and film, based on funding and country imports, provide a further challenge in both providing the service and choice of treatment pathways. Each patient pays 1500 shillings (about 30p) per film which itself is a struggle to find as most are subsistence farmers. This means that nearly all patients only have 1 view on the 1 film.
Together, Moses and I created a method whereby all extremities can be imaged on a single film, regardless of the film size available, with both an AP and lateral view.
The darkroom consists of a single wet tank with developer and fixer and 1 water outlet. The 1 darkroom light was small but worth its weight in gold. Replacement bulbs are difficult to source and in the past Moses has developed films without light for 5 months. A major issue for health and safety of the radiographer was the complete lack of any darkroom ventilation. The hand processed films are mounted on drying racks which are then hung in the film drying cabinet, reliant upon mains power which is limited at best. 20 minutes after arriving in the x-ray room, patients depart carrying their film in a handmade newspaper envelope.
Urgent trauma cases requiring x-rays in times of power outages, are referred to other hospitals in the district, that are at least 2 hours away by car. This is an additional cost that most patients struggle to afford, if at all. The hospital team is extremely generous and during my time on site, I saw several cases where the community of staff pitched in or found a solution for urgent referral costs. Without this support, patients would simply not survive. Engineering maintenance and equipment quality control are reliant on the local hospital engineer, whose tasks also include managing the 1 onsite generator and the entire electrical system including most of the hospital equipment.
X-ray equipment
Current equipment consists of a Siemens Multix Ease fixed over couch x-ray tube, 1 floating top table with under table bucky and 1 erect standalone bucky.
There is no up and down movement of the table, with patients having to climb on to the table. There is no radiopaque mattress, sand bags or foam positioning aids. Whilst we take for granted the technology of the modern NHS, it was the simple things, such as a step, which patients were grateful for in Buluba. From patients with broken bones and leprosy, there was never a complaint, just a smile.
The tube has lateral movement and can be rotated 45 degrees to use with the erect chest stand. There is, however, no horizontal tube movement which results in all patients being pushed or pulled into position on the table. The erect bucky is functional, even though the brake and lock are both broken and as yet there is no spare part available.
Financial constraints in the past year have meant that there was no light beam diaphragm, once the bulb blew, until a replacement was found. This did not interrupt the service provided, as Moses guestimated the light beam diaphragm coverage.
I experienced so many scenarios that radiographers no longer face in the modern CR/DR department and enjoyed every minute of them.
Ultrasound
This service is limited to basic abdominal sonographer and obstetrics, using a Sonoscope Model A6 with variable curvilinear probe 2-7.5 MegaHZ. Currently there is 1 sonographer who visits twice a week. He scans and prepares reports for all patients and works with no breaks. Working with him for 8 hours, I realised he hadn’t even stopped for a drink.
Patients are often alone in the room with the male sonographer and it is not uncommon for them to be naked from the waist up. Men and women alike have no concerns in terms of preserving their dignity or embarrassment at the lack of gowns.
The sonographer was delighted to hear that I was a radiographer, yet dismayed that I was unable to perform ultrasonography, so he set me a challenge to get the new Siemens Sonoline Adara machine operational. This seemed a fair request and the least I could do until I got the power and input sorted and realised that everything was in German. A few tantrums and hours later, we were both pleased to announce that the operational language was now English and the scanner is fully operational. All that is needed now is another full-time sonographer.
I would like to thank the Rotary Doctor Bank, Kerry Bingham, Andy Creeden, Teresa Dawkes, Lucy Foster, Sue Marchant, Angela Ramsay, Christopher Steele, Mansel Thomas, Dr Tim Spare and the tireless devotion of all the staff, visitors and friends in Buluba.
